
TIMS Resources
Quantitative Analysis for MBSS and FEES Using TIMS MVP
Looking to incorporate quantitative measures into your clinical practice?
We’re here to support you.
Quantitative measures have been shown to improve diagnostic accuracy compared with qualitative analysis alone (Kerrison et al., 2023). Standardized approaches further support reproducibility, transparency, reliability, and a consistent patient experience, while promoting clear expectations, the adoption of best practices, and improved patient outcomes (Martin-Harris et al., 2020; Sella-Weiss, 2022).
The tools and scorecards within the TIMS MVP software have been developed and refined to support these goals. This page provides guidance on implementing these tools using TIMS MVP, along with illustrative examples. Implementation should be tailored to each team's needs, expertise, and clinical context. Measurement selection and interpretation should be driven by an integration of theoretical frameworks, research or clinical questions, and clinical expertise.
Important Disclosure: This page provides guidance on selected analysis methods that can be completed using TIMS MVP and is not intended to represent all possible swallowing measures. TIMS MVP does not prescribe or prioritize specific metrics; rather, it offers configurable tools to support diverse measurement approaches. Users are responsible for selecting, implementing, and validating measures in accordance with their study design and scientific objectives.
Quantitative Measures for MBSS, Powered by TIMS MVP
Number of swallows per bolus
Pre-swallow residue
Setting C2-C4 scalar
Peak hyoid movement (using C2-C4 scalar)
Total pharyngeal residue (TPR)
Bolus percentages
Duration of upper esophageal sphincter opening (DUESO)
Laryngeal vestibule integrity
Anatomical changes
Time to laryngeal vestibule closure (LVC)
Duration of laryngeal vestibule closure (LVC)
Maximum Pharyngeal Constriction (PhAMPC)

Number of Swallows Per Bolus
Quick Takeaways
Data obtained when completing the ASPEKT-C Method.
When assessing the number of swallows per bolus using the ASPEKT-C Method, a swallow is defined as UES opening plus at least one of the following: pharyngeal constriction, laryngeal elevation and/or hyoid excursion. Do not include swallow attempts.
Steps for Completion
Use frame-by-frame review with audio on to determine bolus administration.
Track the number of swallows per bolus.
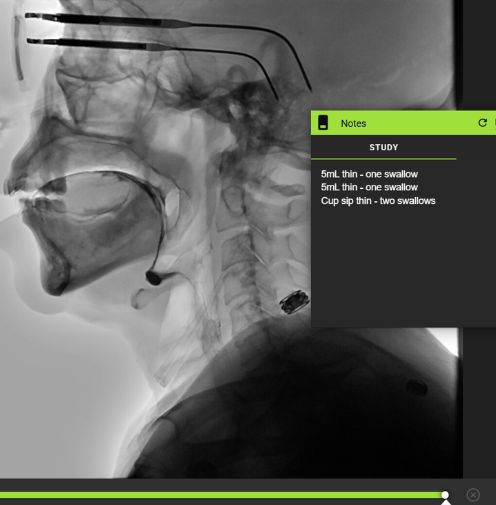
Example: Patient swallowed twice with cup sip thin independently. Data obtained with frame-by-frame review and detailed using the Notes tool.
Pre-swallow Residue
Quick Takeaways
Data obtained when using the ASPEKT-C Method.
Steps for Completion
Record the presence of residue at the beginning of a clip, prior to new material entering the oral cavity.
Note: Compared to clean baseline swallows, those with pre-existing (pre-swallow) residue exceeding consistency-specific thresholds were associated with approximately twice the likelihood of an “atypical” PAS score (≥3) on that swallow (Steele et al., 2020).
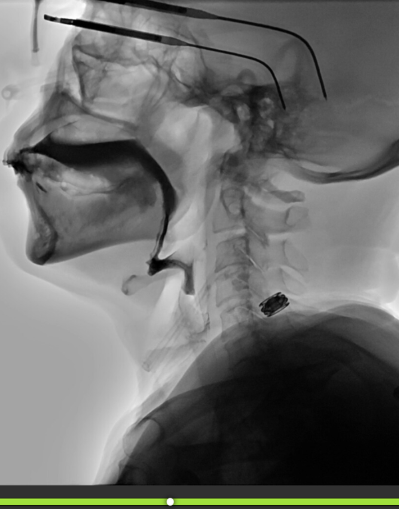
Example: Use of telestrations in TIMS MVP to point out pre-swallow residue.
C2 - C4 Scalar
Quick Takeaways
Scaling measurements to the length of the C2–C4 cervical spine helps account for variability in overall body size, including differences related to sex and height (Molfenter & Steele, 2014).
For some measures, C2-C4 scalar may be used in place of external scalars.
Steps for Completion
Using the line tool, draw a line from the bottom corner of C2 to the bottom corner of C4.

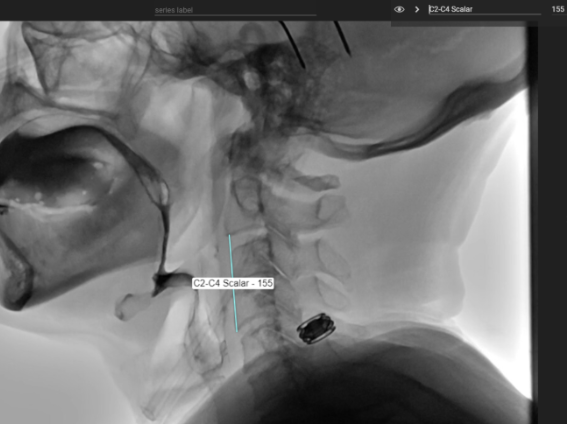
Example: Use of freehand tool to label the spine and use of the line tool to create the C2-C4 scalar.
Peak Hyoid Movement Using the C2 - C4 Scalar
Quick Takeaways
This measure provides the peak hyoid excursion as a percentage of the cervical spine length.
Steps for Completion
Using frame-by-frame review, find the frame of peak hyoid movement.
Set the scalar using the line tool by drawing a line from the bottom corner of C2 to the bottom corner of C4.
Draw a line from the bottom of C4 to the bottom front corner of the hyoid when the hyoid is at its peak movement.
Divide the hyoid movement by the C2-C4 scalar x 100.
Ex. 246/155 = 1.58 x 100 = 158%
This means that the hyoid movement is 1.58 x the length of C2-C4.

Example: Use of the line tool in TIMS MVP to assess peak hyoid movement.
Total Pharyngeal Residue
Quick Takeaways
If there is pharyngeal residue after the swallow of the initial bolus, measure the amount. This data point can be used as described by the ASPEKT-C
Method.
Steps for Completion
Use the line tool to set the C2-C4 scalar.
Using the measurement tool, override the value and set it to 10 pixels. This allows us to create a 10x10 box representative of the C2-C4 squared space. Any subsequent measurements will then be scaled to the C2-C4 scalar (a percentage of 100).
Measure the pharyngeal residue with the freehand tool. TIMS will automatically determine the percentage of residue because of the work you completed with the scalar. The amount you obtain can be compared to the normative data.
In the example below, the pharyngeal residue is 8.42% of the C2-C4 squared space.
Note: By normalizing residue measurements to an individual’s anatomy using the C2-C4 scalar, clinicians can make more meaningful comparisons both within a study and across examinations.
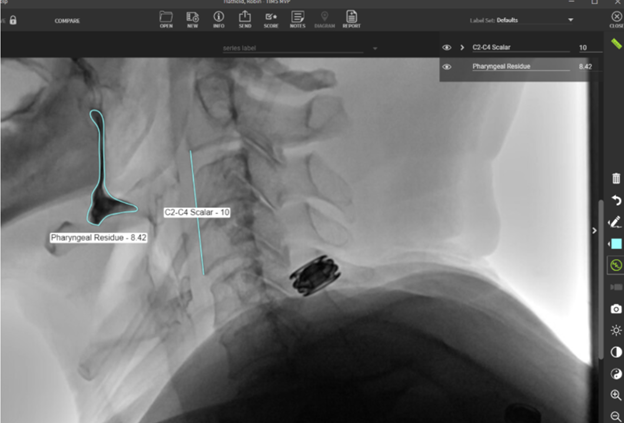
Example: Use of the line and freehand tools to assess TPR in TIMS MVP.
Bolus Estimates
Quick Takeaways
A simple method of analyzing a given bolus.
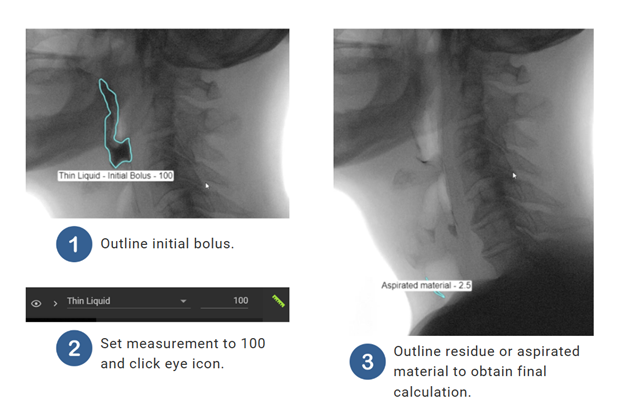
Steps for Completion
Outline the entire bolus prior to UES opening using the freehand tool, magic wand, or magic brush.
Set the measurement to 100%.
Click hide annotation “eye” icon.
Scrub forward to post-swallow, after the UES closes. Outline material you wish to measure (i.e. oral or pharyngeal residue or aspirated material). TIMS MVP will automatically determine the percentage compared to the original bolus.
Duration of Upper Esophageal Opening (DUESO)
Quick Takeaways
DUESO is measured from the moment the UES opens until the moment the UES closes (Robbins et al., 1992, Logemann et al., 2000, 2002). Data is typically obtained in seconds for this measure (Kim, 2009).
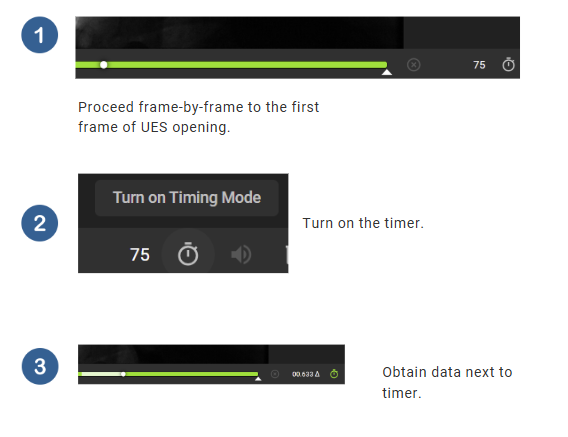
Steps for Completion
Advance frame-by-frame until the first frame of UES opening.
Turn on the timer.
Move forward frame-by-frame until the first frame of UES closure.
Laryngeal Vestibule Integrity
Quick Takeaways
The presence or absence of laryngeal vestibule closure (LVC) can be captured during MBSS analysis. Although this is a dichotomous variable, not a quantitative measure, this physiologic parameter is detailed in this document, given its established importance in airway protection and its contribution to comprehensive swallow analysis when interpreted in conjunction with quantitative measures.
This data point is collected with the ASPEKT-C Method.
Steps for Completion
Using frame-by-frame analysis, review the clip to assess the integrity of the laryngeal vestibule closure.
Determine - was LVC complete or incomplete?
Note: Normative data indicate that complete laryngeal vestibule closure is typical, whereas incomplete closure is atypical.
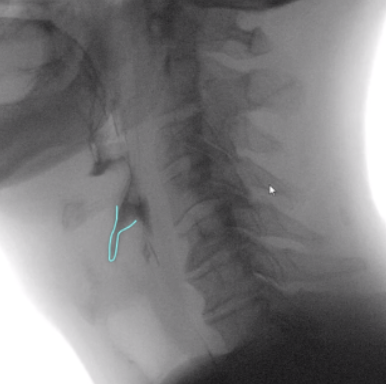
Example: Use of freehand tool in TIMS MVP demonstrating incomplete laryngeal vestibule closure.
Anatomical Changes
Quick Takeaways
Data collected across interventions.
Example scenarios: head and neck lymphedema, anterior cervical disc fusion.
Steps for Completion
Use the line tool to measure the anatomical site you want to assess prior to, and after intervention.
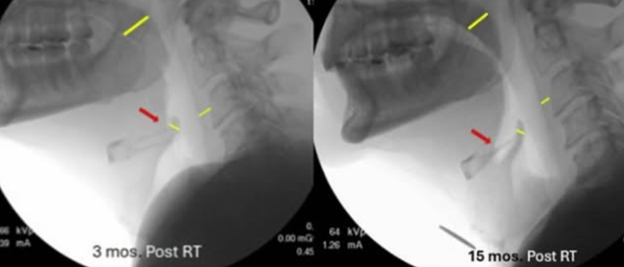
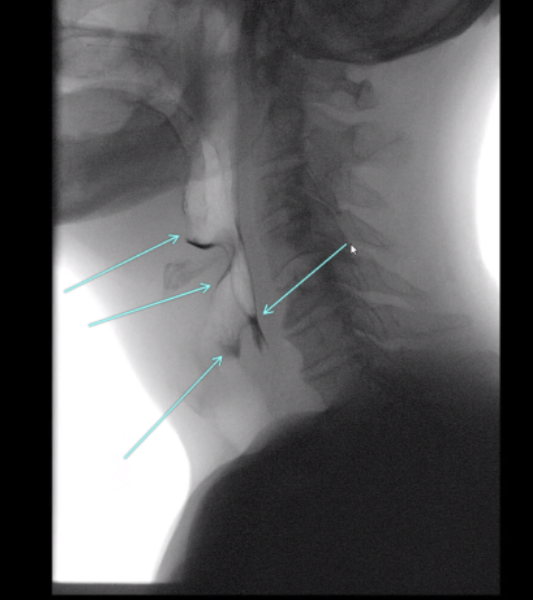
Example: Use of the line tool in TIMS MVP used to assess improvement in three anatomical sites following lymphatic intervention, and a telestration was added to draw attention to the increased vallecular space (Gregor, 2025).
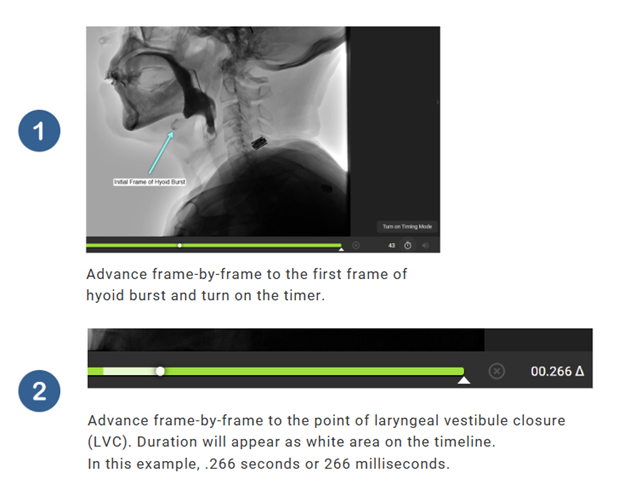
Time to Laryngeal Vestibule Closure (LVC)
Quick Takeaways
Assesses how quickly the laryngeal vestibule closes once the swallow is initiated (Molfenter & Steele, 2012; Vose & Humbert, 2019).
Time to LVC is measured by calculating the time between the first frame of hyoid burst and the first frame of laryngeal vestibule closure.
Typically measured in milliseconds (ms).
Steps for Completion
Use frame-by-frame analysis to find the frame of hyoid burst.
Turn on the timer.
Scrub frame-by-frame until the point of laryngeal vestibule closure (LVC).
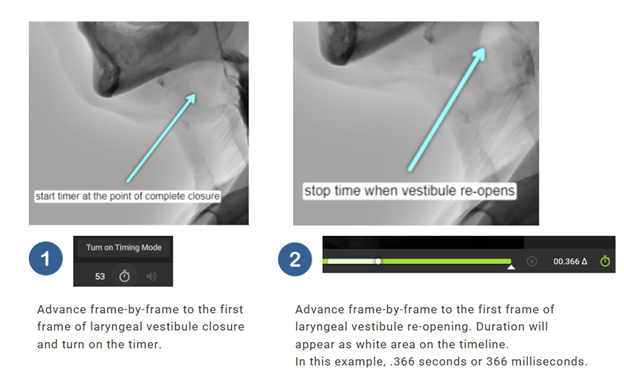
Duration of Laryngeal Vestibule Closure (LVC)
Quick Takeaways
A measure of how long the laryngeal vestibule maintains complete closure (Vose & Humbert, 2019).
Steps for Completion
Using frame-by-frame anlaysis, proceed to the first frame of laryngeal vestibule closure.
Turn on the timer.
Advance frame-by-frame to the first frame of laryngeal vestibule re-opening.
Typically measured in milliseconds (ms).
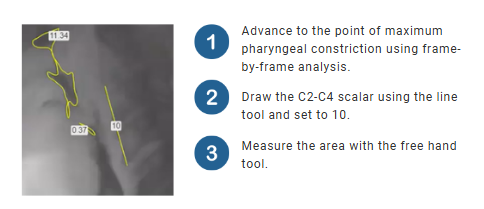
Maximum Pharyngeal Constriction (PhAMPC)
Quick Takeaways
Completed in both ASPEKT and ASPEKT-C.
Assesses how constricted the pharynx is at the height of the swallow.
When selecting the frame of maximum constriction, please note that the frame selected must be before upper pharyngeal relaxation, before tracheal descent, before LVC opening, and before nasopharyngeal relaxation.
When tracing the area, the pharyngeal boundaries are below the top of C2, anterior to the posterior pharyngeal wall, above the UES, posterior to the arytenoids, pharyngeal surface of the epiglottis, and base of tongue.
PhAMPC = Pharyngeal area / (C2-C4 length squared) x 100%.
Please note: When you set the C2-C4 scalar to 10 and complete your tracing, TIMS MVP automatically completes the calculation for you.
Steps for Completion
Using frame-by-frame analysis, advance until the point of max pharyngeal constriction.
Using the line tool, draw the C2-C4 scalar.
Open the measurement tool and set the length of the C2-C4 scalar to 10.
Measure the pharyngeal area at max pharyngeal constriction with the free hand tool. Note: You may have multiple areas as shown below.
Quantitative Measures for FEES, Powered by TIMS MVP
Number of swallows per bolus
Swallow detection
Time to whiteout
Whiteout duration
Total swallow duration
Number of Swallows Per Bolus
Quick Takeaways
Quantifying swallows per bolus provides meaningful, objective data to evaluate swallowing efficiency, guide clinical decisions, and track patient progress over time.
Steps for Completion
TIMS MVP records video and audio simultaneously. If recording the entire FEES without individual clips for each bolus, use frame-by-frame review with audio on to determine bolus administration.
Track the number of swallows per bolus.
Example: If a 15-minute FEES recording is recorded without breaks, TIMS will provide the user with a single recorded clip. Moving the white cursor along the timeline will allow the user to review captured video and audio. The creation of subclips can be beneficial for analysis and archiving purposes.
See the training guide for information regarding subclip creation.
If subclips have been created or individual clips were recorded during the live study, simply use frame-by-frame review to determine the number of swallows per bolus.
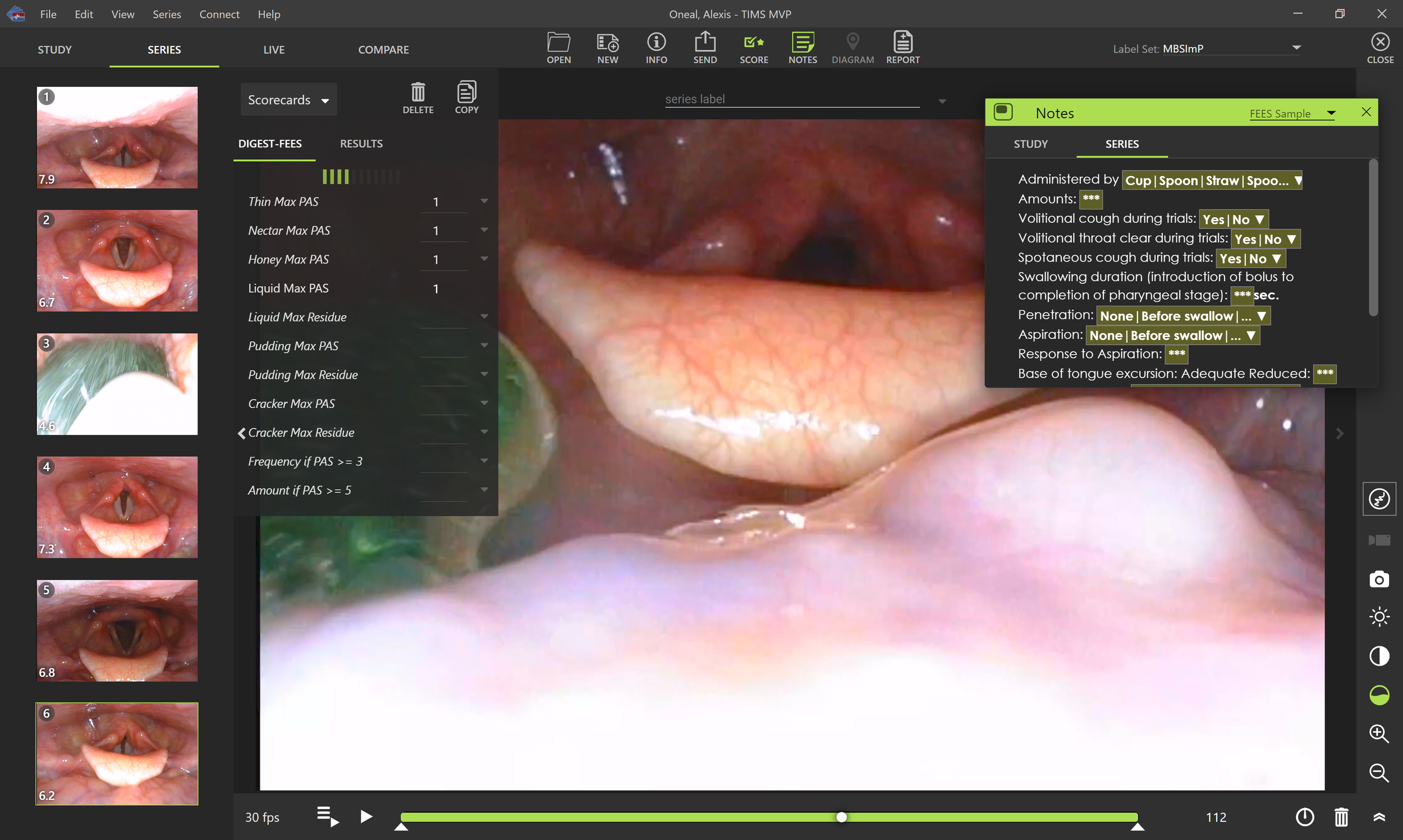
The notes tool can be beneficial for tracking data as you progress through study review.
See photo 2 below.
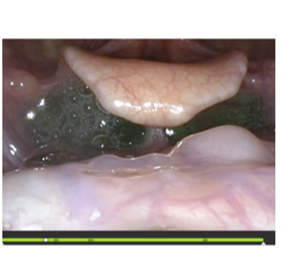
Example: Frame-by-frame review with whiteout detection in TIMS MVP.
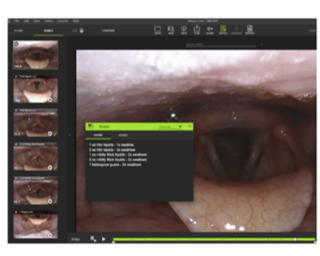
Example: Subclips, notes for data tracking, and use of timeline for frame-by-frame review in TIMS MVP.
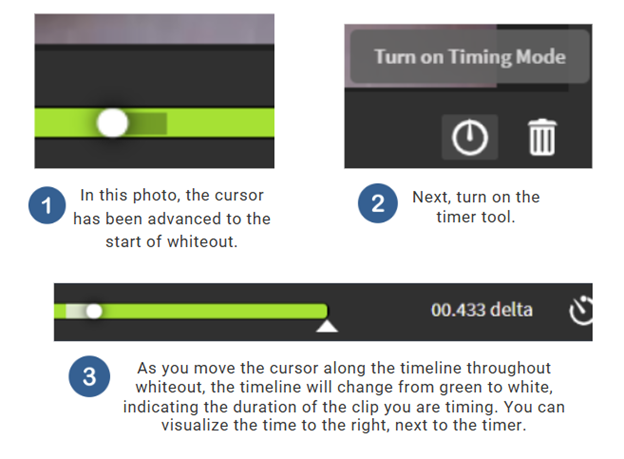
Time to Whiteout
Quick Takeaways
Time to whiteout can be calculated by starting the timer at the first frame after the endoscopist makes a statement regarding bolus presentation and timing until the first frame of complete whiteout.
An example: The bolus is at the lips, and the endoscopist states, “thin liquid bolus presented now.” Reviewing frame-by-frame, the user would determine the first frame after the statement, until the first frame of complete whiteout.
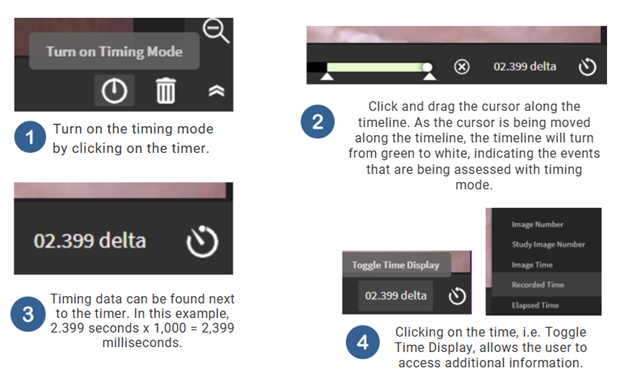
Using the timer tool, a TIMS MVP user can calculate time to whiteout.
Steps for Completion
Click on the timer tool.
Click and drag the cursor along the timeline to measure the duration of the event.
The time will populate next to the timer tool, in seconds.
This data can then be converted to milliseconds by multiplying by 1,000.
Users can also see the frame number adjacent to the duration information.
Duration of Whiteout
Quick Takeaways
Whiteout duration can be calculated using the timer.
Steps for Completion
Using frame-by-frame analysis advance to the first frame of complete whiteout.
Turn on the timer tool.
Click and drag the cursor along the timeline to the first frame that the hypopharynx is visualized to measure the duration of the event.
The time will populate next to the timer tool, in seconds.
This data can then be converted to milliseconds by multiplying by 1,000.
Users can also see the frame number adjacent to the duration information.
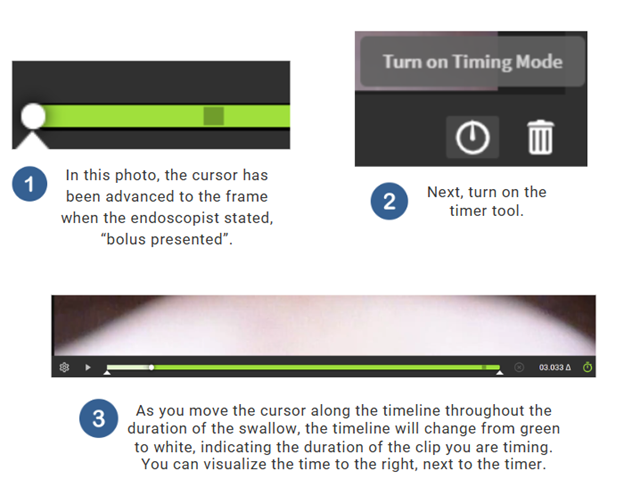
Total Swallow Duration
Quick Takeaways
Total swallow duration can be calculated using the timer.
Steps for Completion
Using frame-by-frame review, scrub forward on the timeline using the cursor to the frame when the endoscopist states, “bolus presented”.
Turn on the timer.
Advance to the first frame when the hypopharynx is visualized after whiteout.
Convert data to milliseconds.
-
Gregor, J. (2025). This patient was diagnosed with T1N2M0 p16+ SCC of the nasopharynx s/p definitive chemoradiation. The left scout is at 3 months post radiation where the patient has developed both external and internal lymphedema of the pharynx and larynx, specifically the velum, posterior pharyngeal wall, and epiglottis [Photograph]. Instagram.
https://www.instagram.com/p/DMZLv5DxNjN/Langmore, S. E. (2001). Endoscopic evaluation and treatment of swallowing disorders. Thieme.
Kerrison, G., Miles, A., Allen, J., & Heron, M. (2023). Impact of quantitative videofluoroscopic
swallowing measures on clinical interpretation and recommendations by speech-language
pathologists. Dysphagia, 38(6), 1528–1536. https://doi.org/10.1007/s00455-023-10580-3Kim, Y (2009). Temporal and biomechanical measurements of upper esophageal sphincter
(UES) opening in normal swallowing. Korean Journal of Communication Disorders, 14, 109-
116.Leonard, R. (2017). Two methods for quantifying pharyngeal residue on fluoroscopic swallow
studies: Reliability assessment. Annals of Otolaryngology and Rhinology, 4(3), 1168–1171.Leonard, R., Miles, A., & Allen, J. (2023). Bolus clearance ratio elevated in patients with
neurogenic dysphagia compared with healthy adults: A measure of pharyngeal efficiency. American Journal of Speech-Language Pathology, 32(1), 107–114.
https://doi.org/10.1044/2022_AJSLP-22-00199Logemann, J. A. (1998). Evaluation and treatment of swallowing disorders. Austin, TX: Pro-
ed.Logemann, J. A., Pauloski, B. R., Rademaker, A. W., & Kahrilas, P. J. (2002). Oropharyngeal
swallow in younger and older women. Journal of Speech, Language, and Hearing Research, 45,
1-12.Martin-Harris, B., Canon, C. L., Bonilha, H. S., Murray, J., Davidson, K., & Lefton-Greif, M. A.(2020). Best practices in modified barium swallow studies. American Journal of Speech-Language Pathology, 29(2S), 1078–1093. https://doi.org/10.1044/2020_AJSLP-19-00189
Molfenter, S. M., & Steele, C. M. (2013). Variation in temporal measures of swallowing: sex
and volume effects. Dysphagia, 28(2), 226–233. https://doi.org/10.1007/s00455-012-9437-6Molfenter, S. M., & Steele, C. M. (2014). Use of an anatomical scalar to control for sex-based size differences in measures of hyoid excursion during swallowing. Journal of Speech, Language, and Hearing Research, 57(3), 768–778. https://doi.org/10.1044/2014_JSLHR-S-13-0152
Robbins, J., Hamilton, J. W., Lof, G. L., & Kempster, G. B. (1992). Oralpharyngeal swallowing in normal adults of different ages. Gastroenterology, 103, 823-829.
Rommel, N., Borgers, C., Van Beckevoort, D., Goeleven, A., Dejaeger, E., & Omari, T. I. (2015).Bolus residue scale: An easy-to-use and reliable videofluoroscopic analysis tool to score bolus residue in patients with dysphagia. International Journal of Otolaryngology, 780197.https://doi.org/10.1155/2015/780197
Sella-Weiss, O. (2023). The test of mastication and swallowing solids and the timed water swallow test: Reliability, associations, age and gender effects, and normative data.International Journal of Language & Communication Disorders, 58(1), 67–81.
https://doi.org/10.1111/1460-6984.12768Smaoui, S., Peladeau-Pigeon, M., & Steele, C. M. (2022). Determining the relationship between hyoid bone kinematics and airway protection in swallowing. Journal of Speech, Language, and Hearing Research, 65(2), 419–430. https://doi.org/10.1044/2021_JSLHR-21-00238
Steele, C. M., Peladeau-Pigeon, M., Barrett, E., & Wolkin, T. S. (2020). The risk of penetration-aspiration related to residue in the pharynx. American Journal of Speech-Language Pathology,29(3), 1608–1617. https://doi.org/10.1044/2020_AJSLP-20-00042
Sutton, S., Lim, L., Servino, K., To, H., Wang, L., McCoy, Y., Bice, E. M., & Galek, K. E. (2024). Normal values for swallow events during endoscopic evaluation of swallowing: A preliminary study. European Archives of Oto-Rhino-Laryngology, 281(10), 5517–5525. https://doi.org/10.1007/s00405-024-08782-y
Vose, A., & Humbert, I. (2019). "Hidden in Plain Sight": A descriptive review of laryngeal vestibule closure. Dysphagia, 34(3), 281–289. https://doi.org/10.1007/s00455-018-9928-1